April 2015
For Enquiries and Appointments call +91 97136 11611 (Pune Centres) | Akluj: 02185-224444
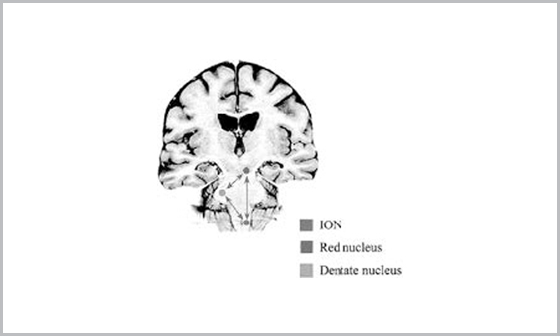
Small, well-defined T2 and flair hypointensity involving the left paramedian pons which shows blooming on the gradient images with punctate enhancement on post contrast study–consistent with residual pontine cavernoma.Associated developmental venous anomaly noted with prominent veins coursing in the midline through the pons and across the left middle cerebellar peduncle. Left olivary nucleus of medulla shows hyperintense signal without significant swelling. No diffusion restriction/presence of blood degradation products is seen. No e/o enhancement is noted.
Hypertrophic olivary degeneration – postoperative sequelae of pontine cavernoma resection