September 2013
For Enquiries and Appointments call +91 97136 11611 (Pune Centres) | Akluj: 02185-224444
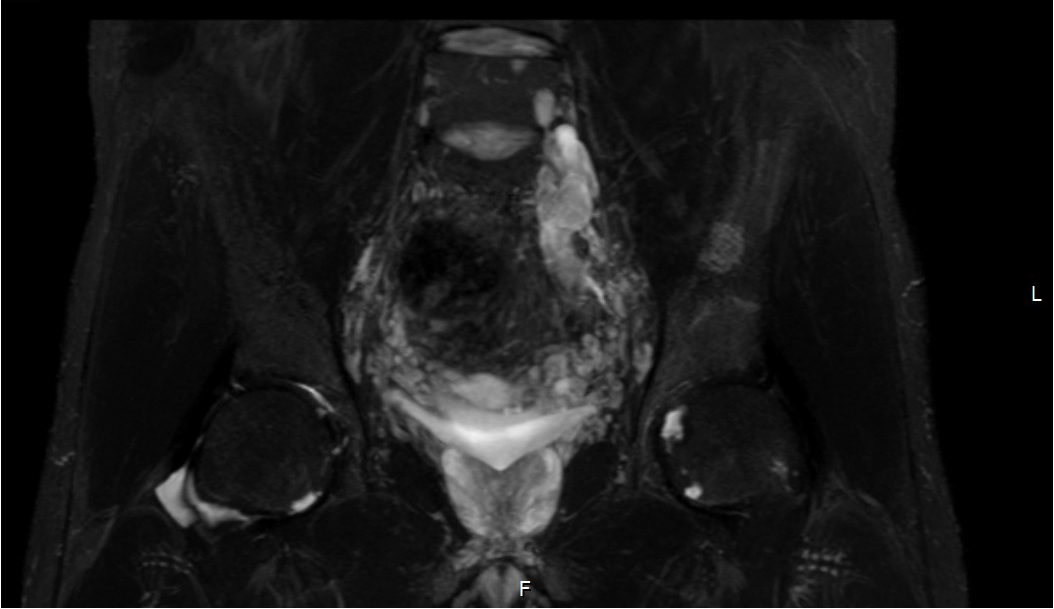
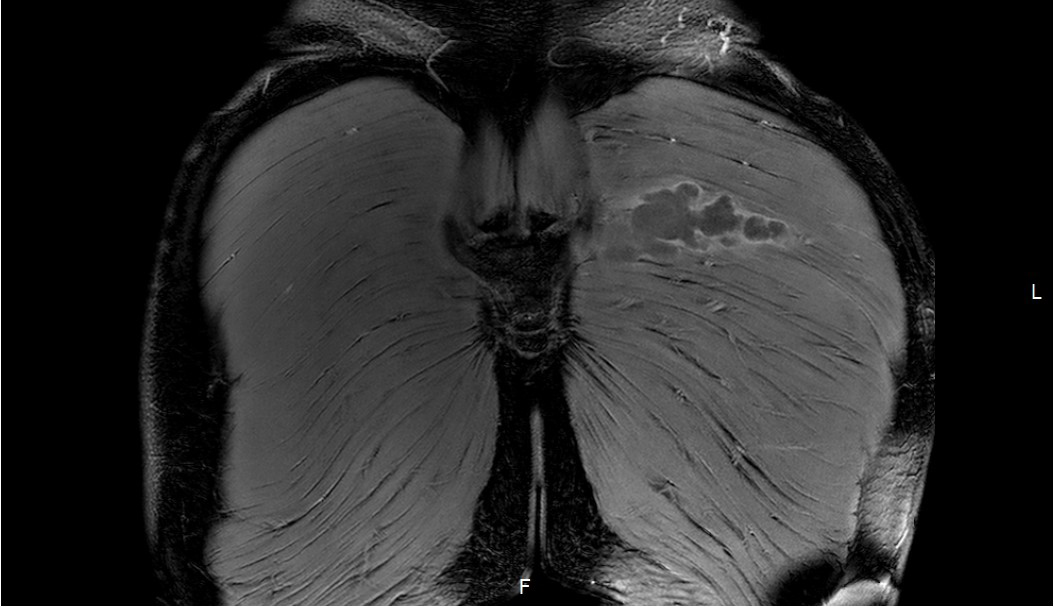
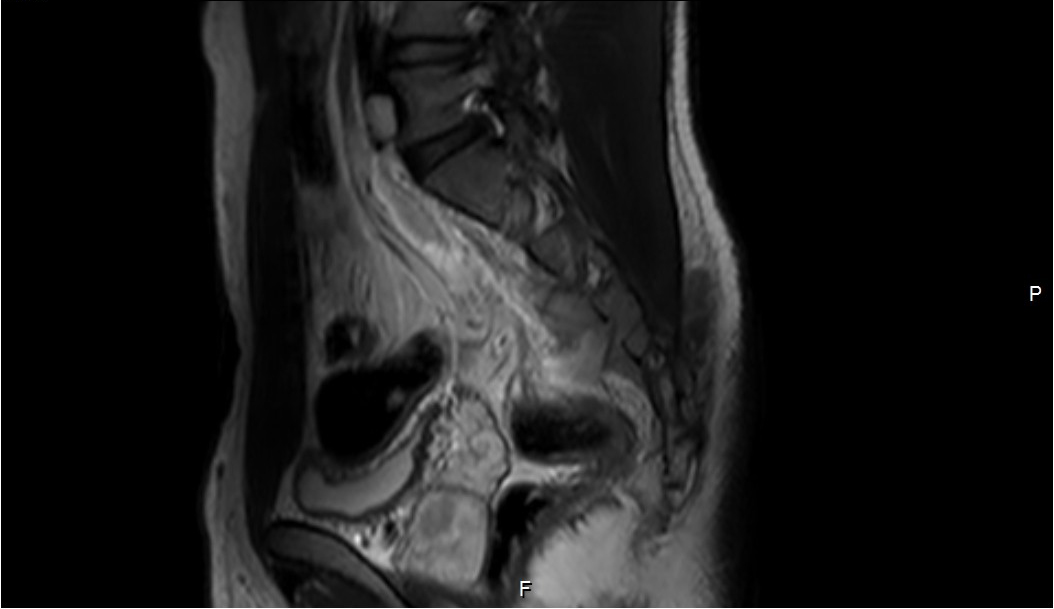
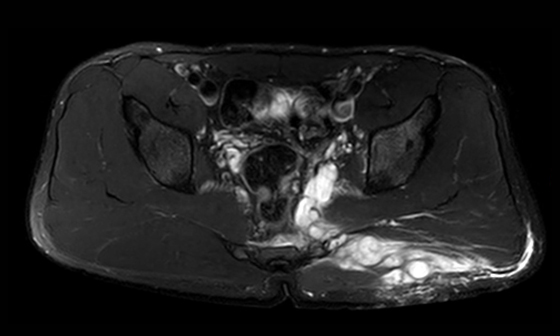
Large lobulated T2-hyperintense sol in the presacral space from of L5 level downwards along the lumbosacral nerve plexus with intrapelvic (medial to the sciatic nerve along the internal iliac vessels involving the lower sacrum on left side from S2 to S4 levels upto the midline) portion and large extra-pelvic extension along the superior border of the pyriformis muscle through the upper portion of the greater sciatic notch into the left gluteal region (along superior gluteal nerve) upto the subcutaneous fat. Mild heterogeneous enhancement of the intrapelvic portion is noted with the gluteal portion showing minimal peripheral enhancement (cystic). Normal left sciatic nerve is visualised antero-inferior to the lesion below the pyriformis muscle.
Multiple conglomerate nerve sheath tumors (schwannomas) with intra and extra pelvic (dumbbell) components.
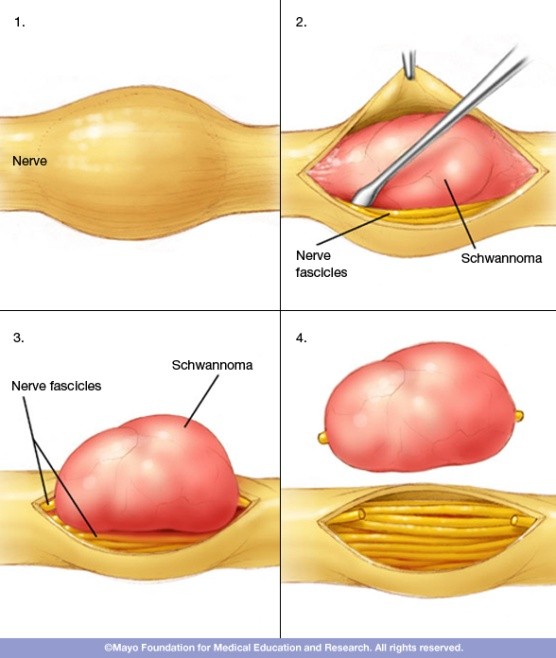
Schwannoma
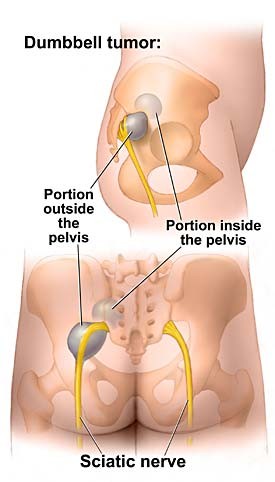
These include schwannomas and neurofibromas, tumors that form within the nerve. Most are round and small. Others may enlarge and assume unusual shapes, such as dumbbell tumors in spine and pelvis.
The most common benign peripheral nerve tumor in adults. It typically comes from a single bundle (fascicle) within the main nerve and displaces the rest of the nerve. When more fascicles are involved, a schwannoma grows larger, making removal more difficult. In general, they grow slowly.
Schwannoma most frequently affects patients 20 - 50 years of age and accounts for approximately 5% of all benign soft tissue neoplasms. Men and women are affected equally.
Although the head and neck, the flexor surfaces of the extremities (particularly the ulnar and peroneal nerves), and the mediastinum and retroperitoneum represent the most common sites of involvement, schwannomas can occur almost anywhere. Pain and neurologic symptoms are uncommon unless the lesion is large.
Schwannomas present as fusiform, well-defined masses that rarely exceed 5 cm in diameter. Continuity with a nerve is usually best seen in lesions arising from larger nerves and is virtually diagnostic. The distinction of schwannomas and neurofibromas by the position of the tumor relative to the nerve (eccentric versus central) is often difficult; it can be best appreciated on axial MR images when a large peripheral nerve is involved.
These reveal isointense signal relative to skeletal muscle on T1-weighted images and increased, slightly heterogeneous signal intensity on T2. They show variable enhancement patterns.
THOROUGH WORK-UP OF AN INNOCUOUS SUBCUTANEOUS SWELLING IS SOMETIMES REQUIRED ESPECIALLY WHEN RECURRENT
These reveal isointense signal relative to skeletal muscle on T1-weighted images and increased, slightly heterogeneous signal intensity on T2. They show variable enhancement patterns.
--- IT CAN WELL BE JUST THE ‘TIP OF ICEBERG’.