March 2014
For Enquiries and Appointments call +91 97136 11611 (Pune Centres) | Akluj: 02185-224444
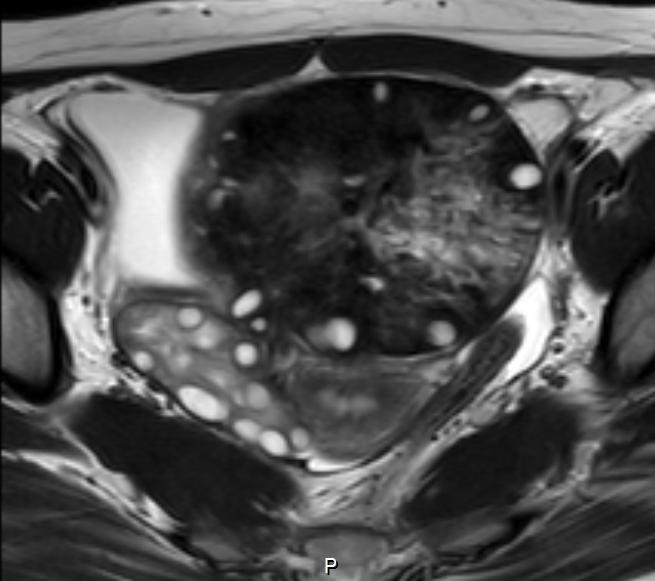
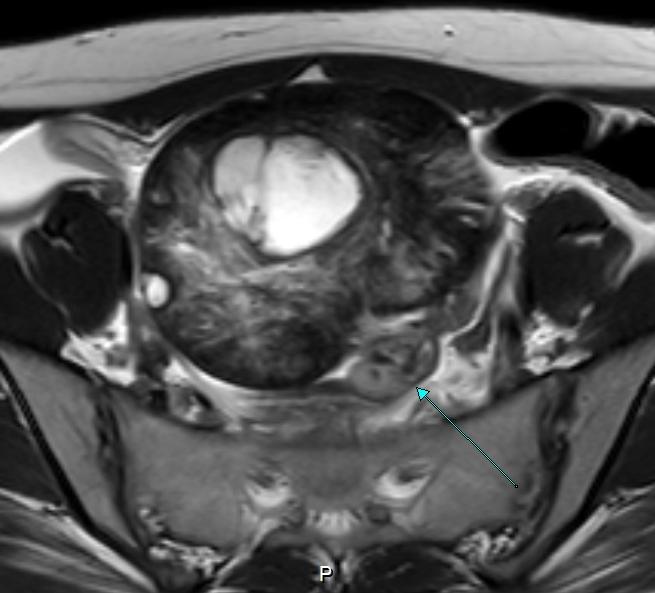
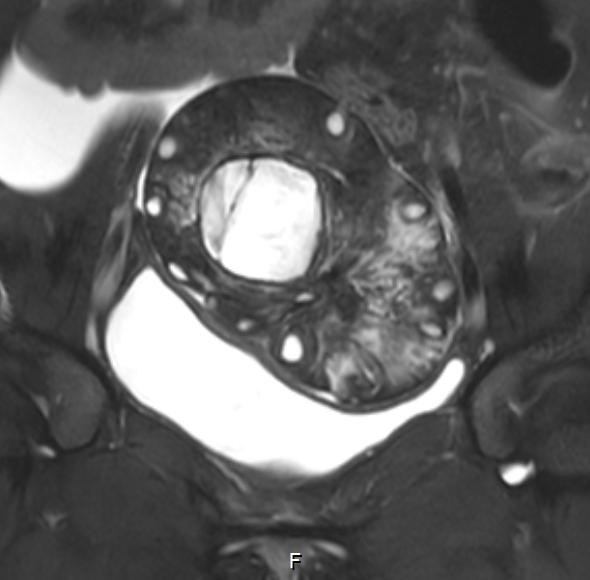
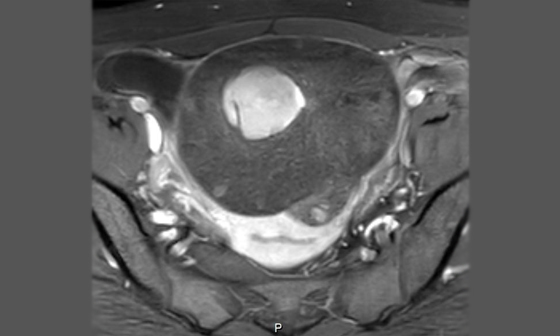
Large, predominantly hypointense lesion on T2 and STIR images in the left adnexa (not separately seen from the left ovary). Heterogeneous hyperintense areas are also seen within the lesion along with multiple small round to oval cysts in the periphery. The cysts show hyperintense fluid signal on T2W images. Minimal hyperintensity is seen within the cystson T1w images, with the rest of the lesion appearing isointense on T1W images. Minimal to absent enhancement after administration of contrast was seen. The central portion of the lesion shows a hemorrhagic component measuring 38x32 mm; it is bright on all sequences and not suppressed with fat saturation. Limited CT images do not show evidence of calcification in the lesion. There is a thickened tubular structure along the posterior aspect of the lesion, showing post contrast wall enhancement. The right ovary is bulky and shows multiples mall peripheral cysts with cenral stroma–polycystic. It also shows a 13x12 mm hemorrhagic cyst in its superior portion.
Ovarian torsion is defined as partial or complete rotation of the ovarian vascular pedicle and causes obstruction to venous outflow and arterial inflow. Ovarian torsion is usually associated with a cyst or tumor, which is typically benign; the most common is mature cystic teratoma.
Ultrasonography (US) is the primary imaging modality for evaluation of ovarian torsion. US features of ovarian torsion include a unilateral enlarged ovary, uniform peripheral cystic structures, a coexistent mass within the affected ovary, free pelvic fluid, lack of arterial or venous flow, and a twisted vascular pedicle. The presence of flow at color Doppler imaging does not allow exclusion of torsion but instead suggests that the ovary may be viable, especially if flow is present centrally. Absence of flow in the twisted vascular pedicle may indicate that the ovary is not viable.
Common CT features of ovarian torsion include an enlarged ovary, uterine deviation to the twisted side, smooth wall thickening of the twisted adnexal cystic mass, fallopian tube thickening, peripheral cystic structures, and ascites.
Enlarged ovary with a central afollicular stroma (resulting from hemorrhage and edema) and peripherally displaced follicles is a specific feature.
Uterine deviation due to mass effect from an enlarged ovary is an associated feature of torsion. The most common lesion associated with a torsed ovary is a physiologic follicular or corpus luteal cyst, dermoid, cystadenomas fibromas, and Brenner cell tumors, ovarian malignancy, including carcinoma, germ cell tumors Sertoli Leydig cell tumors, and metastases.
Twisted pedicle.
Subacute ovarian hematoma/hemosalpinx.
Abnormal enhancement after IV contrast agent administration. Heterogeneous minimal or absent enhancement indicates the evolution of ovarian torsion from ischemia to infarction.