October 2014
For Enquiries and Appointments call +91 97136 11611 (Pune Centres) | Akluj: 02185-224444
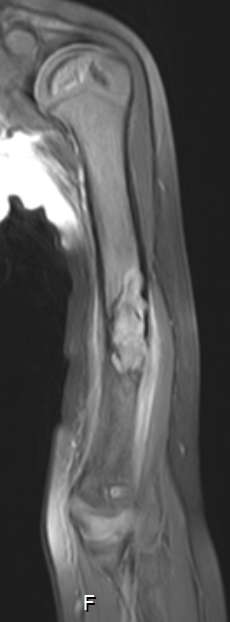
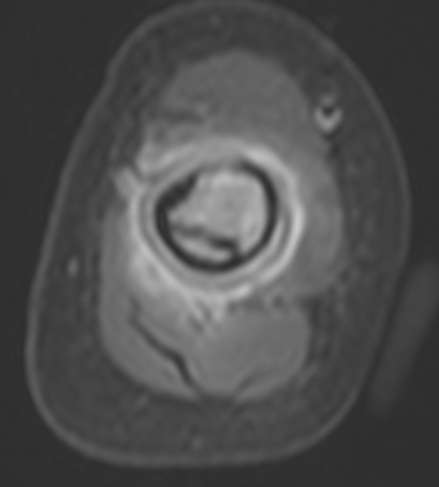
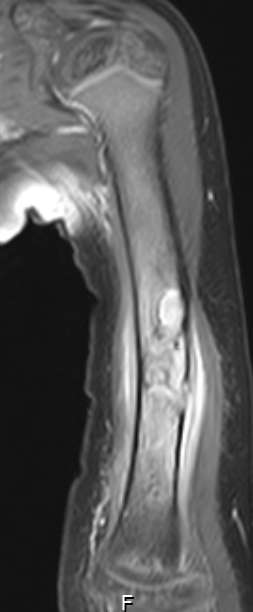
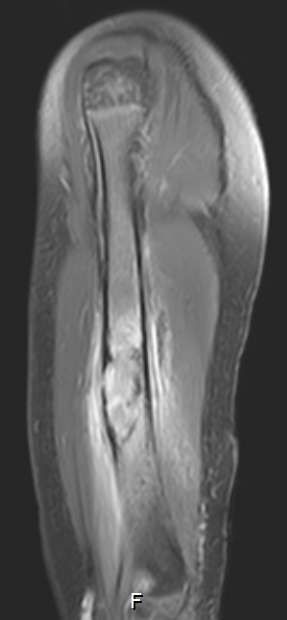
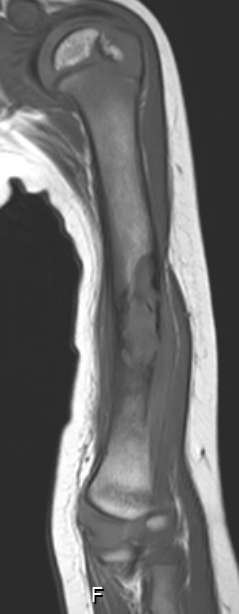
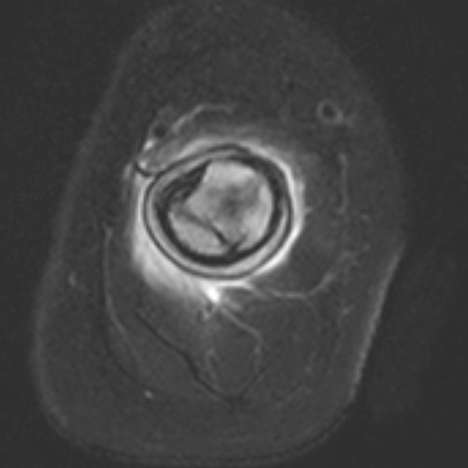
Considering MRI findings-
Irregular area of altered marrow signal intensity in diaphyseal location with cortical break and associated periosteal thickening and adjacent paraosseous soft tissue.
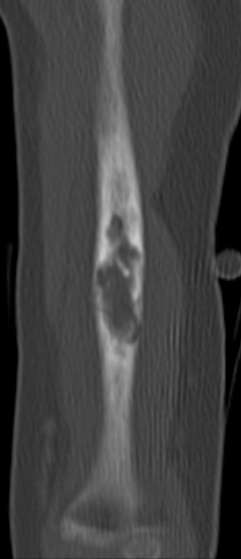
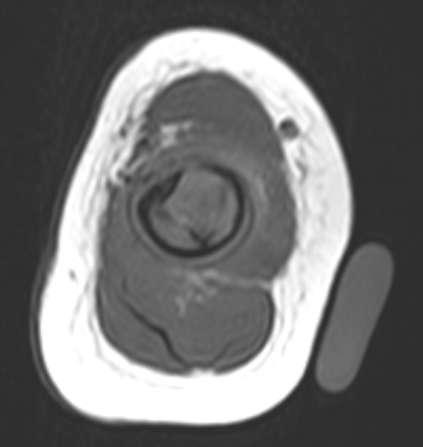
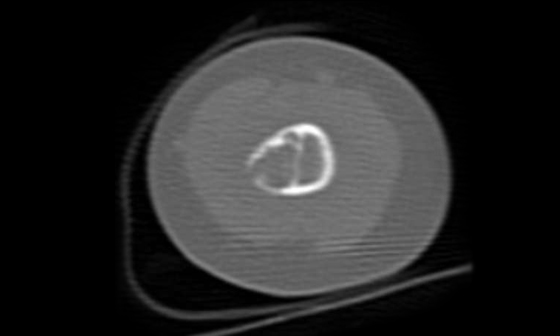
Considering CT findings –
Cortical and diaphyseal location of lesion.
Bowing of shaft of humerus.
Peripheral sclerotic margin.