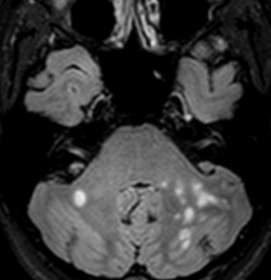
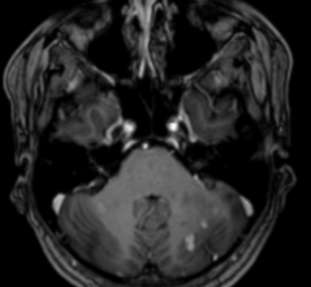
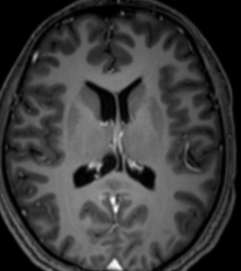
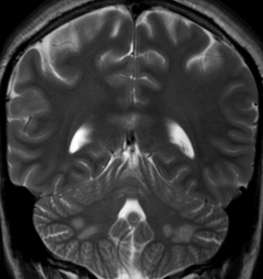
Multiple focal T2 hyperintense foci were seen in the posterior fossa involving the pons and the cerebellar white matter. There was asymmetrical affection. Punctuate/nodular and a few linear areas of enhancement were seen on post contrast study
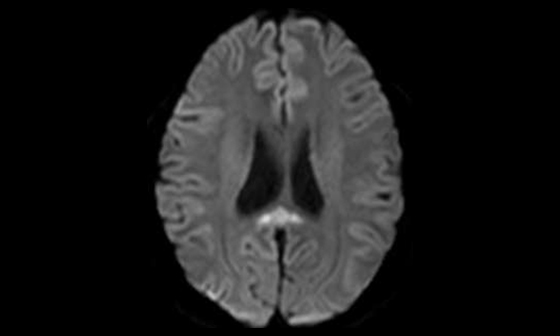
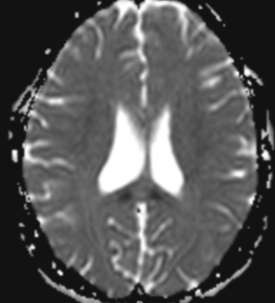
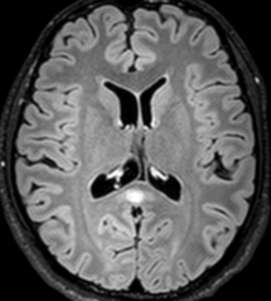
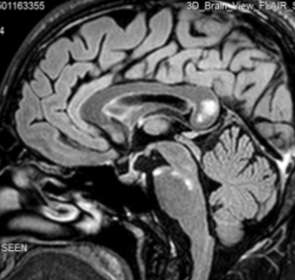
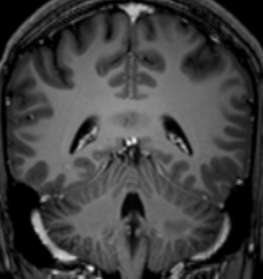
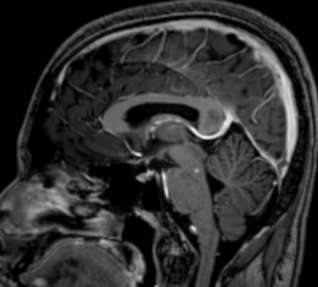
Affection of the central part of corpus callosum was also noted. Lesion was diffusion restricted in parts and did not enhance on the postcontrast study. Callososeptal interface was normal
Susac’s syndrome is a rare disease of unknown pathogenesis
Caused by a microangiopathy affecting the arterioles of the brain, retina, and cochlea, giving the classic clinical triad of subacute encephalopathy, visual loss secondary to retinal branch occlusions, and sensorineural hearing loss
MR imaging, retinal fluorescein angiography, and audiography findings enable diagnosis
Most cases of Susac’s syndrome occur in young, healthy women, aged 18–40 years
The disease usually has an active fluctuating monophasic self-limited course, lasting from months to years, with varying functional outcomes and residual disabilities
The etiology and pathogenesis of this microangiopathy remains unknown
Various treatments have already been used: corticosteroids, an immunosuppressive agent (Cyclophosphamide), antiplatelets, antithrombotic agents, intravenous immunoglobulins, plasmapheresis, and hyperbaric oxygen
It appears that in patients in whom diagnosis and treatment are delayed, permanent morbidity is higher in terms of neurologic deficit, visual loss, and hearing loss. Rapid and early therapy should reduce sequelae of this disease
A high index of suspicion must be present because a high percentage of patients as many as 97%do not have the clinical triad at the time of onset of symptoms
The triad may become complete after a delay of weeks to more than 2 years, and partial forms of the syndrome have been reported, making the diagnosis more difficult
Susac syndrome can mimic several diseases. The differential diagnosis includes any disorder that can produce multifocal neurologic symptoms, visual impairment, hearing loss, or any combination of these and is therefore very large: demyelinating disease, connective tissue disease, infection, neoplasm, procoagulant state, and ischemic disease of different etiologies
Possibility of Susac’s syndrome should be suspected in any adult or young patient presenting with acute/subacute encephalopathy with or without visual or auditory symptoms and T2 bright white matter lesions with corpus callosal affection at brain MR imaging
Rapid diagnosis is important as early therapy may reduce sequelae and improve recovery
Tai Hung Do, Christiane Fisch, Francois Evoy Susac Syndrome: Report of Four Cases and Review of the Literature AJNR 2004 ;25: 382-388
Susac JO, Hardman JM, Selhorst JB. Microangiopathyof the brain and retina. Neurology 1979;29:313–316
Ayache D, Plouin GI, Bakouche P, et al. Microangiopathy of the inner ear, retina, and brain (Susac syndrome): report of a case. Arch Otolaryngol Head and Neck Surg 2000;126:82–84
Susac JO. Susac’s syndrome: the triad of microangiopathy of the brain and retina with hearing loss in young women. Neurology 1994;44:591–593