Hand and Foot Imaging at Star
VOL. 8 .NOVEMBER-DECEMBER 2013 CLINICAL NEWSLETTER
Dear Colleague,
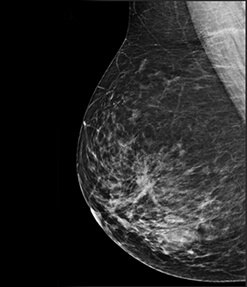
Our second venture is now fully operational at Connaught Place, Bund Garden Road. It houses state of the art facilities like 3Tesla MRI with Ambient experience, 64 Slice Brilliance Cardiac CT Scanner, High resolution USG with 3D & 4D facilities & computerised radiography. And now, we are proud to introduce South East Asia's First and Only Full Field Digital Mammography with Tomosynthesis and advanced Breast Intervention to the city of Pune. We take this opportunity to welcome Dr. Varsha Hardas who specialises in Breast Imaging & Dr. Sonali Deshmukh to our STAR FAMILY.
Evaluation of hands and feet has always posed a challenge from a clinical as well as radiological perspective. Imaging of these regions is tricky due to presence of numerous, small and compactly arranged structures. MRI has been the preferred imaging modality.However with the advent of 3T & use of dedicated coils for small structures like fingers it is possible to resolve extremely thin &small structures as never before.
In this newsletter we intend to demonstrate how use of 3T MRI & dedicated imaging coils facilitate imaging of various pathologies of hands& feet.
Dr. Sanjay Desai, Dr. Ashish Atre
Case 1 - Plantar Fibromatosis
Courtesy: Dr.Govind Marathe, Dr.Sanjay Sane
Clinical presentation -
Case 1: A 62 year old woman came with history of chronic pain along the plantar aspect of the foot worsening on walking. Radiographs were not contributory.
Case 2: A 64 year old lady came with similar clinical picture.

Review of Literature
Plantar fibromatosis (Ledderhose disease) occurs most frequently between the ages of 30-50 years with male predilection. Bilateral involvement and concomitant palmar fibromatosis are common.
These lesions develop most commonly in the medial aspect of the plantar aponeurosis and manifest as one or multiple firm, fixed,subcutaneous nodules and but are often asymptomatic.
On MR imaging, they are typically poorly defined (infiltrative) or rarely localised occurring in the deep aponeurosis adjacent to the plantar muscles in the medial aspect of foot. They have heterogeneous signal intensity equal to or less than that of skeletal muscle on both T1- and T2-weighted spin-echo MR images and show variable enhancement.
Imaging Interpretation Pearls
Fibrous tumors show signal intensity less than the skeletal muscle on all sequences. Even when seen in atypical locations / age / sex, their signal characteristics are typical enough to warrant attention and aid in prompt diagnosis.
Case 2 – Enchondroma
Courtesy: Dr. Chetan Pradhan
Clinical presentation - A 27 year old lady came with history of swelling and discomfort over the index finger of left hand. Radiographs showed expansile lesion in the second metacarpal, possibly enchondroma.

Review of Literature
Enchondromas are relatively common benign medullary cartilaginous neoplasm, usually found in children or young adults (10- 30 years). They are usually asymptomatic, but may be complicated by a pathological fracture or after rare malignant transformation into a low grade chondrosarcoma.
Almost all enchondromas are intra-medullary with small tubular bones of hands and feet accounting for 50% of them. They may arise from the metaphysis but are more commonly seen in diaphysis.
MRI is useful in evaluating for soft tissue extension and confirming the diagnosis. Enchondromas are well circumscribed, show intermediate to low signal on T1, are extremely bright on T2 (due to mature hyaline cartilage) and show variable enhancement. Focal regions of T2-signal drop out suggest calcifications. Typically, there is no bonemarrow or soft tissue edema.
DD: Low grade chondrosarcoma, bone infarct, intraosseous ganglion, epidermoid inclusion cyst, metastasis, granulomatous disease (sarcoidosis /)
Imaging Interpretation Pearls
Expansile medullary lesion with cortical thinning, bright signal on fluid-sensitive sequences, central punctuate calcification and sharp demarcation from normal marrow are characteristic of cartilage containing tumors.
Although radiographs best predict a type of bone neoplasm, MRI is extremely important in detecting an early malignant change in the form of associated soft tissue abnormality.
Case 3 - Spina Ventosa
Courtesy: Dr. Sandeep Patwardhan
Clinical presentation - A 12 year old girl came with history of swelling and pain over the ulnar aspect of the hand since 2 months. Expansile lesion in the fifth metacarpal with cortical breaks raised the possibility of enchondroma with fractures.

Review of Literature
Tuberculous dactylitis (also known as spina ventosa) is a skeletal manifestation of tuberculosis [spina = short bone and ventosa = expanded with air]. Tuberculous osteietis is one of the commonest bacterial osteitis and typically affects pediatric age group. It involves the short tubular bones of the hands and feet and often follows a benign course without pyrexia and acute inflammatory signs.
DD: pyogenic / fungal infections, syphilitic dactylitis, sarcoidosis, hyperparathyroidism
Imaging Interpretation Pearls
An intramedullary lesion with surrounding sclerosis / cortical thickening and extra-osseous soft tissue abscesses should raise the suspicion of infection – especially tuberculosis in the Indian setting.
Case 4 - De Quervain's Tenosynovitis
Courtesy: Dr. Umesh Joshi
Clinical presentation - A 23 year old man came with history of pain along the proximal aspect of thumb

Review of Literature
De Quervain tenosynovitis is a painful stenosing tenosynovitis involving the first extensor (dorsal) tendon compartment of the wrist (typically at the radial styloid) which contains the and extensor pollicis brevis (EPB) tendons.
It usually occurs in middle-aged individuals and is around 3 times more common in women with most cases related with overuse.
Patients present with pain on thumb and wrist movement and with focal tenderness and swelling over the radial styloid. As APL and EPB tendons are tightly secured against the radial styloid by the overlying extensor retinaculum in a fibro-osseous tunnel, any thickening / fluid restrains normal gliding movements. Presence of an intertendinous septum between the tendon worsens the prognosis.
MRI is very sensitive and specific for the diagnosis and extremely helpful in detection of intertendinous septum.
DD: Tenosynovitis related to inflammatory arthropathies such as rheumatoid arthritis, intersection syndrome
Imaging Interpretation Pearls
Identification of the tendon (APL / EPB) abnormality must be primarily at the level of radial styloid although it may extend proximo-distally.
Case 5 - Giant Cell Tumor of Tendon Sheath
Courtesy: Dr. Pankaj Jindal
Clinical presentation - A 24 year old woman came with history of painful swelling and movements ofthe index finger of the right hand.

Review of Literature
A giant cell tumor of the tendon sheath (GCTTS) is an uncommon and usually benign lesion that arises from the tendon sheath. It is also known as pigmented villonodular tumor of the tendon sheath (PVNTS).
Clinically, they typically present in the hand (although found elsewhere) with localised swelling with or without pain and are slow growing. Typically, they present in 3rd-5th decades and have a slight female predilection.
Given their histological similarity to PVNS, GCTs of the tendon sheaths also share the same findings on MRI, mainly on account of hemosiderin accumulation. They exhibit low signal on both T1 and T2WI and show variable enhancement.
DD: Desmoid tumor, fibroma, ganglion cyst, glomangioma.
Imaging Interpretation Pearls
Any soft tissue lesion with dark areas on T2 or gradient images, PVNS should be the top differential.
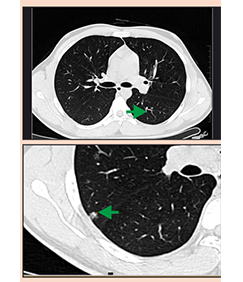
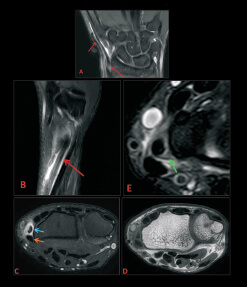
Case 6 - Hand Vascular Malformation
Courtesy: Dr. S. Prashanth
Clinical presentation - A 38 year old man came with history of painful, slowly increasing swelling in the palm of the hand since 2000.

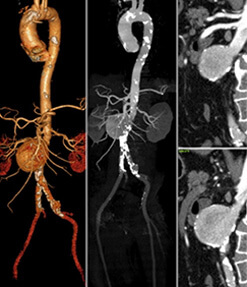
Utility of CT: CT Images show tiny foci of calcification indicative of phleboliths – confirmatory for low flow vascular (venous) malformation.
Review of Literature
Venous malformations, formerly referred to as hemangiomas, are the commonest vascular soft tissue abnormality comprising 7% of benign soft tissue tumors.
As terminology for vascular anomalies is confusing and inconsistent, classification has been developed by the International Society for the Study of Vascular Anomalies (ISSVA) based on clinical, radiological, hemodynamic and histological criteria.
Group 1 - Vascular tumors due to vascular proliferation --- hemangiomas (infantile or congenital).
Group 2 - Vascular lesions due to inborn errors in morphogenesis --- vascular malformations (low flow and high flow).
Combining STIR sequences with time-resolved (dynamic) contrast-enhanced 3D MR angiography is capable of providing exact delineation and accurate characterization of congenital vascular malformations in the extremities; sufficient to confidently plan therapeutic interventions.
On STIR images, vascular malformations are fluid-filled and extremely bright against a dark background of other tissues. It is also easy to detect\ muscular and bony involvement.
The present implementation of dynamic contrast-enhanced 3D MR angiography provides limited flow information. Temporal resolution (images C, D & F) separates the different vascular phases and thus accurately classifies lesions and delineates feeding and draining vessels.
Imaging Interpretation Pearls
MR imaging with STIR & dynamic CE sequences is the mainstay of imaging of venous malformations. It is the single best modality to detect, characterize and stage venous malformations.
Case 7 - Thenar SOL
Courtesy: Dr. Abhijeet Wahegaonkar, Dr. Anil Bhatia
Clinical presentation - A 34-year-old man came with history of slowly growing slightly painful swelling in the 1st webspace.

Review of Literature
Fibrolipomatous hamartoma (lipoma of the nerve) is related to hypertrophy of mature fat and fibroblasts in the epineurium. It presents in young adults with a slow growing mass, usually on volar aspect of the hand. It has marked predilection for the median nerve and may give rise to pain / paresthesia.
The MR appearances are typical with longitudinally oriented cylindrical foci of low signal intensity surrounded by fat signal giving a 'spaghetti' appearance on coronal and 'coaxial cable' appearance on the axial images. On MRI areas of low and high signal intensity areseen on both T1 and T2-weighted images are present in the fibrous and fatty contributions of the tumor.
Imaging Interpretation Pearls
Presence of SOL with fat and fibrous tissue along the distribution of a nerve prompts the diagnosis of a fibrolipoma especially when typical 'spaghetti' or 'coaxial cable' appearances are appreciated.
Finger Injuries
Important normal anatomy

Case 8 to 11 - Spectrum of finger injuries
A.Extensor Tendon Injury
Courtesy: Dr. Swapnil Bhalgat
Clinical presentation - A 50 year old man came with history of 'mallet' deformity of little finger secondary to trauma.
Review of Literature
Normal anatomy overview: The extensor tendons at the MCP joint are stabilised over the dorsum of the metacarpal head by the extensor hood especially the sagittal bands. Distal to the MCP joint, the extrinsic and intrinsic tendons blend into the dorsal apparatus circumferentially distributed over the dorsum of the fingers. The extrinsic and intrinsic tendons form the central and lateral slips inserting into the middle and distal phalanx respectively.
Injuries:Extensor tendon injuries can be either open or closed. Mallet finger is a type of closed injury. It results from a lesion of the bony or ligamentous attachment of the extensor mechanism to the distal phalanx with resultant incomplete extension of the DIP joint. If untreated it progresses to a swan-neck deformity caused by retraction of the extensor mechanism.
The sagittal plane best allows identification and confirmation of the diagnosis. Bony avulsions are also identified in few patients.

B. Pulley Injuries
Courtesy: Dr. Abhijeet Wahegaonkar
Clinical presentation -A 49 year old woman came with history of fixed flexion deformity of index finger secondary to trauma few years back with h/o surgical repair at that time.
Review of Literature
Normal anatomy overview: From the neck of the metacarpal to the DIP joint, the flexor tendons of the individual fingers run along osteofibrous canals line by a synovial sheath.
The fibrous portion of the canal consists of 5 annular pulleys (A1-A5) which are transverse areas of thickening of the tendon sheath and 3 cruciform pulleys (C1-C3) which are from by criss-crossing fibres of the components of the annular pulleys.
Injuries:Lesions of the pulley system are being increasingly recognised. These injuries usually begin in the distal A2 pulley (the most important component in the flexor tendon function), progressively involving the A3, A4 and rarely the A1 pulleys.
Early diagnosis and accurate assessment of pulley tears is essential for choosing between conservative management and surgery that can prevent fibrous sequelae and flexion contracture of the PIP joint.
MRI shows useful indirect signs like detection of gap between the flexor tendon and the bone on sagittal images obtained during forced flexion – 'bowstringing sign'.
High resolution axial MR sections allow direct visualisation of the normal and disrupted pulleys disrupted A2 and A4 pulleys, obviating the need for imaging with forced flexion to demonstrate indirect signs.

C. Collateral Ligament Injuries
(i) Level - PIP Joint (Bicondylar Joint)Courtesy: Dr. Abhijeet Wahegaonkar
Clinical presentation -A 38 year old woman came with history of pain in the region of PIP joint of little finger with limitation of movements secondary to trauma 4-5 months back.

(ii) Level - MCP Joint (Unicondylar Joint)
Courtesy: Dr. Abhijeet Wahegaonkar
Clinical presentation- A 27 year old man came with history of painful movements and feeling of instability in the region of MCP joint of ring finger.

Review of Literature
Normal anatomy overview: Collateral ligaments are one of the main stabilisers of the proximal interphalangeal and metacarpophalangeal joints along with the volar plate.
The collateral ligament complex consists of the collateral ligament proper, accessory collateral ligament and volar plate (fibrocartilaginous structure along the volar aspect of joint capsule).
Injuries:The PIP joint is the most commonly injured joint in the hand. Its injuries are further classified according to the plane of resultant instability - coronal and sagittal.
Although the supporting structures of the MCP and PIP joints are similar, the unicondylar nature of the MCP joint allows significant radial and ulnar deviation as well as some rotation. Volar plate is interconnected with the adjacent MCP joints by the deep transverse metacarpal ligament. Volar plate and the sagittal bands of the extensor tendon also contribute to joint stability.
Collateral ligament injuries can be demonstrated in acute (discontinuity / detachment / edema hemorrhage) with or without leakage of synovial fluid and chronic (thickening with scar formation / thinning / wavy contour) stages.
Imaging Interpretation Pearls
Thorough knowledge of the anatomy of the small structures is essential in correct diagnosis of the injuries and their prognostication. High resolution MRI with dedicated coils play an unprecedented role in accurate interpretation of their injuries and accurate surgical planning.
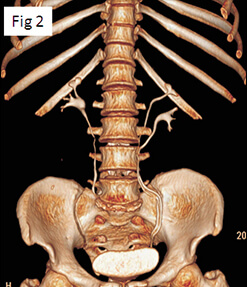
Case 12 – Melorheostosis
Courtesy: Dr. Arun Salunke
Clinical presentation - A 20 year old man came with chronic pain along the lateral aspect of his left foot with stiffness on walking.

Review of Literature
Melorheostosis [melos (limb); rhein (to flow)] is a rare form of mixed sclerosing bone dysplasia of obscure etiology. In young adults, irregular ossification is seen along the outer cortex, mimicking candle drippings.
Patients with melorheostosis may develop secondary symptoms related to limitation of motion, joint fusion, or periosteal irritation. It is usually monomelic and involves one or more segmental sclerotomes (innervated from individual spinal sensory nerve) of lower limbs.
Despite characteristic features, atypical presentations raise uncertainties about the diagnosis and are difficult to differentiate from chronic ostemylelitis.
Most of the clinical signs are associated with fibrosis causing joint stiffness, angular joint deviations and contractures (mostly flexion).
DD: Chronic osteomyelitis, periosteal osteosarcoma, myositis ossifications, reflex sympathetic dystrophy, neurofibromatosis, metastases.
Imaging Interpretation Pearls
Plain radiographs are characteristic but may not be available at the time of MRI in most patients. Hence, when MRI of foot shows hyperostosis and hypointensities along a sclerotome in the appropriate clinical setting. melorheostosis has no differentials.
Case 13 - Tarsal Coalition
Courtesy: Dr. Abhishek Andhare
Clinical presentation - A 60-year-old woman came with history of chronic worsening pain in the foot on activity. She had flatfoot since many years.

Review of Literature
Tarsal coalition describes complete / partial union (developmental fusion) between two or more bones in the mid or hindfoot. It excludes acquired conditions (rheumatoid arthritis, trauma or postsurgical). It may be of bony, cartilaginous or fibrous varieties.
It occurs in about 6% of the population and although congenital,patients typically present by adolescence. There is a significant male predilection (M:F 4:1) with upto 50% bilaterality. Pes planus (fixed flat foot) is usually a common feature.
Vast majority (90%) of tarsal coalitions are either calcaneonavicular or talocalcaneal.Plain films in many instances yield the diagnosis of bony coalition, if strongly suspected and carefully evaluated. Other types are commonly missed.
MRI is the modality of choice to look for all 3 types of coalition. It also shows associated findings secondary to the condition namely marrow or soft tissue oedema and arthritic changes. Multislice CT is confirmatory in bony coalitions.
Imaging Interpretation Pearls
Tarsal coalition must be strongly suspected and looked for in every case of flat foot, especially if fixed. Careful evaluation of the radiographs and MRI are required for the correct diagnosis, especially in the cartilaginous / fibrous varieties.