Cardiac Imaging at Star Imaging and Research Centre
Dr. Preeti Neve/ Dr. Ashish Atre
Structural as well as functional cardiac abnormalities and coronary artery disease have traditionally been evaluated in the past using catheter angiography and Doppler / echocardiography studies.
It is now possible to evaluate coronary artery disease with high level of accuracy in a non-invasive manner using multidetector CT scanners (MDCT). CT coronary angiography has a high negative predictive value and is also very useful to evaluate post-therapy patients (ie.depiction of revascularisation after stent placement and CABG surgeries).
Cardiovascular magnetic resonance imaging (MRI) has evolved from an effective research tool into a clinically proven, safe andcomprehensive imaging modality.
In this issue we would like to showcase cardiac MRI imaging studies and applications performed at Star Imaging centre. A dedicated cardiac imaging coil and postprocessing software at Star allow for multiple applications in evaluating myocardial infarction and viability, imaging the cardiomyopathies and cardiac masses. Lack of ionising radiation, excellent spatial resolution, 3D anatomical assessment and ability to provide tissue characterisation with and without contrast are few of the many advantages of Cardiac MRI making it a valuable and complementary tool to other non-invasive modalities.
Cardiac MR Viability imaging allows differentiation ofreversible versus irreversible myocardial injury, transmural extent ofinfarction and detects associated microvascular obstruction. These factors help risk stratification and are important prognostic indicators in predicting response to therapy and hence serve as guiding principles for the appropriate revascularistion procedure.
First-pass magnetic contrast myocardial perfusion is fast becoming a superior alternative to radionuclide techniques for the detection of coronary atherosclerotic disease.
Cardiovascular MRI is the “gold standard” for quantifying ventricular volumes, ejection fraction and myocardial mass.
In acute chest pain syndromes with unobstructed coronaries Cardiac MRI has the unique capability of discriminating infarction from myocarditis or cardiomyopathy aiding in the clinical management of these patients.
Cardiac MRI is also useful in the work-up of all patients with suspected cardiomyopathy due to its ability to study the right ventricle, to detect subtle wall motion abnormalities or reduction in LVEF.It can also detect myocardial oedema and small areas of fibrosis or scarring.
This modality also allows for repeated imaging / screening of patients with a family history of cardiomyopathy and in athletes who experience unexplained syncope or aborted sudden cardiac death syndrome.
Case 1:
Courtesy: Dr. NITIN PATKI
Clinical Presentation:
Chest discomfort in a known hypertrophic cardiomyopathy patient.
To evaluate coronary tree.
CT coronary angiography was performed followed by DSA and stenting.
A subsequent one year follow up CT coronary angiography was performed.

Case 2:
Courtesy: Dr. M S HIREMATH
Clinical Presentation:
History of MI, angiography with stenting was performed for revascularisation.
Follow up imaging.



Case 3:
Courtesy: Dr. M S HIREMATH
Clinical Presentation:
Post CABG status.
Chest pain with positive stress test results


Review of Literature
• Cardiac coronary angiography study allows ostium evaluation, presence/absence of vascular remodelling, percentage stenosis, characterisation of the plaque, evaluation of its extent and site, involvement of branch origin and evaluation of distal vessel. Limitations include very high calcium deposition within the vessel walls obscuring the lumen due to blooming artifacts.
• It has a negative predictive value in the range of 98% for ruling out significant instent restenosis.
• Assessment of bypass grafts and distal runoffs by invasive coronary angiography is cumbersome and often requires extra procedure time, contrast load, and radiation exposure. Cardiac CT provides 3D anatomy of grafts, is noninvasive and successfully visualises the grafts, anatomosis and distal vessel.
CMR - MYOCARDIAL VIABILITY IMAGING
Case 4:
Courtesy: Dr. SHIREESH SATHE
Clinical Presentation
Coronary angiography: triple vessel disease. Culprit vessel LAD.
Study indication: Viability to decide for revascularisation procedure.




Case 5:
Courtesy: Dr. M S HIREMATH
Clinical Presentation:
History of AMI in 2009.
Study indication: Viability for prognosis.

Review of Literature:
Myocardial infarction is typically caused by luminal thrombosis superimposed on coronary atherosclerosis. Occasionally it can be caused by coronary spasm, coronary embolism, or thrombosis in nonatherosclerotic vessels.
Irreversible injury of ischemic myocardium progresses as a wavefront, occurring first in the subendocardial myocardium but ultimately becoming transmural.
In MI, regional wall-motion abnormalities of the affected vascular territory can be seen on cine images. T2-weighted images show wall thickening / thinning and myocardial edema. If there is irreversible damage, hyperenhancement is seen on delayedenhancement images along the distribution of the involvedepicardial coronary artery.
Imaging Interpretation Pearls
Cardiac MR Viability imaging allows documentation of reversible versus irreversible injury, transmurality of infarction and associated phenomenon of microvascular obstruction. These factors help risk stratification and are important prognostic indicators predicting response to therapy. In triple vessel disease CMR can identify the culprit vessel and also guide appropriate revascularisation procedure.
Also evaluation of complications such as aneurysm formation, intraventricular thrombosis, papillary muscle and valvular involvement can be assessed.
CMR – CARDIOMYOPATHY HOCM
Case 6:
Courtesy: Dr. M S HIREMATH
Clinical Presentation:
Chest Pain.
Coronary angiography: Normal.
2D echo suggestive of ventricular hypertrophy.



Review of Literature
Hypertrophic cardiomyopathy (HOCM) represents most common cause of sudden cardiac death in young. Abnormal EEG associated with marked asymmetrical septal hypertrophy and a dynamic LVOT obstruction is almost diagnostic. Typical patterns of LGE are patchy or confluent, generally confined to segments with greatest wall thickening and at the RV-LV insertion points. Septal thickness exceeding 30 mm is one of the risk factors for adverse prognosis.
CMR – CARDIOMYOPATHY ARVD
Case 7:
Courtesy: Dr. J S HIREMATH
Clinical Presentation:
10 year old child
Dyspnoea on exertion.
2D echo suggestive of dilated right heart chambers and significantly dilated RVOT.
RIGHT VENTRICLE FUNCTIONAL ANALYSIS
Right ventricular function: (RVEF 19.7%).
The functional SA, RV analysis are as follows:
ED volume 97.4 ml
ES volume 78.2 ml
EF volume 19.7%
Stroke vol. 21 ml



Review of Literature
Arhythmogenic right ventricular dysplasia (ARVD) is an inherited condition predominantly involving the right ventricle with progressive loss of myocytes and fibrofatty tissue replacement. Dilated right ventricle associated with ventricular arrhythmias is common clinical presentation.Diagnosis relies largely on the ARVC task force criteria. Major criteria that can be documented on CMR include regional wall motion abnormality / dyskinesia documented by Cine images of the right ventricle and globally reduced right ventricular function with right ventricle ejection fraction less than 40%. Pattern of LGE is non-specific though can contribute to delineate different patterns of a ARVC.
Imaging Interpretation Pearls
CMR offers potential for high spatial resolution images with excellent border definition allowing accurate measurements of peak wall thickness especially in the apical and basal anteroseptal wall variants of HOCM, which are more difficult to image with echo. Degree of LVOT obstruction and presence of systolic anterior motion of the mitral valve can be quantified. CMR can provide important clue to differential diagnosis of secondary left ventricular hypertrophy.
CMR is an integral component of clinical evaluation and represents the gold standard for assessing the right ventricle.
CMR- MYOCARDITIS
Case 8:
Courtesy: Dr. J S HIREMATH
Clinical Presentation:
History of ventricular ectopic.
Coronary angiography is normal.





Review of Literature
Clinical presentation of myocarditis could vary from simple flu like illness to troponin positive chest pain, heart failure and sudden cardiac death. On MRI, in acute stage, oedema appears as regions of increased signal intensity on T2/STIR images. Early gadolinium enhancement in areas of T2 hyperintensity reflects tissue hyperaemia. LGE identifies acute inflammation and areas of irreversible necrosis in later stages, typically affecting the subepicardium and sparing the subendocardium. Mid wall LGE is also characteristic for viral myocarditis.
Imaging Interpretation Pearls
Delayed-enhancement imaging is the most important technique and accurate method for evaluation of chest pain syndromes with pattern of enhancement allowing differentiation of ischemic versus nonischemic cardiomyopathies, myocarditis and pericarditis.
CMR – CARDIAC MASSES – LEFT VENTRICULAR MYXOMA
Case 9:
Courtesy: Dr. ABHIJEET JOSHI / Dr. RANJEET JAGTAP
Clinical Presentation:
Mild chest discomfort. History of syncope.
2D echo suggestive of intraventricular lesion.




Review of Literature
Myxomas are the most common type of primary cardiac tumour. They are typically solitary, and have a predilection for the interatrial septum near the fossa ovalis. Intraventricular myxoma is relatively rare. Cine imaging is very useful in the work-up of myxomas as they are highly mobile, occasionally prolapsing through the mitral valve and causing obstruction. The treatment is surgical resection with a margin of normal tissue and is considered curative.
Imaging Interpretation Pearls
CMR has become a highly valuable technique offering incremental value owing to its larger field of view, superior tissue contrast, versatility in image planes, and unique ability to enable discrimination of different tissue characteristics, such as water and fat content, which give rise to particular signal patterns with T1- and T2-weighted techniques. With contrast material– enhancedMR imaging, additional tissue properties such as vascularity and fibrosis can be demonstrated. MR imaging can therefore contribute to the diagnosis of a cardiac mass as well as be used to detail its relationship to other cardiac and extracardiac structures. These assessments are important to plan therapy, such as surgical intervention.
NON-CONTRAST MR ANGIOGRAPHY OF THE ABDOMINAL AORTA AND LOWER LIMB ARTERIES
Case 10:
Courtesy: Dr. D. Kamerkar
clinical Presentation:
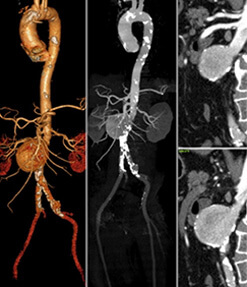
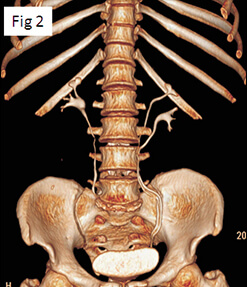
A 59 yr old patient with h/o diabetes mellitus, and complaints of bilateral lower limb claudication. He underwent contrast enhanced CT angiography as well as non-contrast 2D TOF MR angiography of the abdominal aorta and lower limb arteries.

Images and imaging findings:
CE-CTA and NC MRA images of infra-renal abdominal aorta and the lower limb arteries:
1. Left femoro-popliteal artery occlusion with collaterals, well seen on both NC MRA and CE CTA images. ( )
2. Infrapopliteal arterial segments show diffuse disease, bilaterally with mixed calcific plaques on CTA. NC MRA well demonstrates the flow underlying these plaques. ( )
Review of Literature
Peripheral arterial disease continues to be a major cause of morbidity and mortality, with an increasing prevalence in the elderly population.
With the advent of multidetector row CT, CTA has emerged as a reliable, noninvasive alternative to DSA. The limitations of MDCT angiography include difficulties in evaluation of severely calcified vessels due to beam hardening artifacts, risk of exposure to ionizing radiation and the use of iodinated contrast media.
MR angiography without use of any intravenous contrast medium at high field strength MRI (3T), has evolved as an useful competing imaging modality for evaluation of these patients.
Imaging Interpretation Pearls
Non contrast MR Angiography is a non-invasive, cost–effective, OPD technique, to evaluate peripheral arterial disease. Besides, there is no exposure to ionizing radiation .It can be safely done in patients with renal insufficiency and in those with hypersensitivity to contrast media.
Recently concluded study at STAR IMAGING & RESEARCH CENTRE, comparing Non Contrast MR angiography with contrast enhanced CT angiography has shown MR angiography to be superior to CTA in evaluation of calcified vessels distal to popliteal artery. This is awaiting Publication in Journal of Vascular Surgery published by Elsevier for society for vascular surgery.