128 slice CT Scanner at Star Imaging and Research Centre
Dr.Preeti Neve/Dr. Ashish Atre
STAR imaging and research centre was started with a dream of providing worldclass diagnostic facilities to one and all. The latest and high end machines are backed by an equally competent team of radiologists with speciality imaging as the most unique feature which is how founder and director Dr. Ashish Atre had envisioned it.
Recent installation of premium 128 Slice Ingenuity CT at STAR Imaging centre is an important milestone in realizing our mission with improved diagnostic results at markedly reduced and lowest possible radiation exposure.
Philips unique Adaptive multi cycle reconstruction algorithm achieves temporal resolutions as fast as 53 milliseconds which leads to excellent quality images with faster acquisition times. These features put us at an advantage for imaging the vascular system from head to toe and also in paediatric cardiac CT studies.
Moreover it is also equipped with award winning iDose4 technology which ensures t
CT AORTA ANGIOGRAPHY

Case 1:
Courtesy: Dr.PramodNarkhede and Dr.Makhale
Clinical Presentation
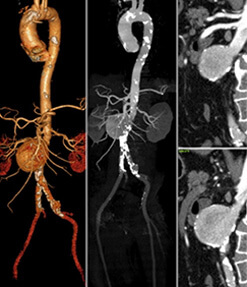
History of abdominal aorta aneurysm on regular USG follow up. Pre and posttreatment aorta angiography imaging.
Type-II-endoleak-into-the-aneurysm-sac-from-collateral-supply-through-IMA.-IMA-fills-from-the-SMA-through-Artery-of-Drummond.

Case 2:
Courtesy: Dr. Rahul Sheth and Dr. Bharat Dalvi

Clinical Presentation:
Coarctation of aorta treated with surgical grafting. Now presented with hemoptysis. Diagnostic Thoracic aorta angiography was done followed by endovascular repair. Follow up imaging.
REVIEW OF LITERATURE
• CT aorta angiography study allows optimal evaluation of aorta with respect to course, caliber, plaque evaluation, involvement of branch vessel origin, distal vessel. Simultaneous evaluation of end organ has an additive role.
• Post endovascular / surgical repair assessment is an important area where CT provides 3D anatomy, isnoninvasive and successfully evaluates all associated complications within and outside the vascular lumen.
• 128-slice MDCT scanner offers better diagnostic interpretation and display of the entire aorta non-invasively and at lowest radiation dose (iDose).
CT CAROTIDANGIOGRAPHY
Courtesy: Dr.Ravindra Kadam
Clinical Presentation :
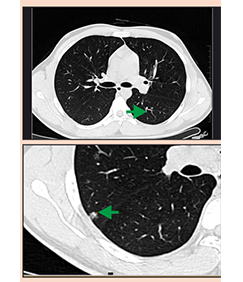
In a 43 yr old man with acute non-hemorrhagic infarct involving the right lentiform and right temporal and parietal lobes on the recent plain CT brain scan. He underwent contrast enhanced CT angiography of the neck and intracranial arteries.
Imaging Findings
• Plain CT brain images show acute non-hemorrhagic infarct in the right lentiform and right temporal and parietal lobes (a).
• The axial and coronal MIP (b, c) and volume rendered (VRT) images (d, e): reveal a non-calcific atherosclerotic plaque (arrows) at the right carotid bifurcation extending into right proximal internal carotid artery (ICA), causing mild (about 30%) luminal stenosis.

Review of Literature
One of the key diagnostic elements guiding the therapeutic approach in the acute phase of an ischemic stroke is the presence or absence of intracranial large vessel occlusion (LVO). This can be detected using neurovascular CTA of the head and neck.
CTA, being a non-invasive technique saves both procedure time and patient discomfort, as compared with DSA and MRA. It provides high quality, three dimensional image data sets to study cerebro-vascular anatomy
CT RENAL ANGIOGRAPHY
Case:Renal FocalLesion Evaluation
Courtesy: Dr. N.N. Bapat
Clinical Presentation:
A 50 yr old woman camewith complaints of pain onthe left side of abdomen.

Review of Literature
In staging renal cell carcinoma, the goal of any imaging study is to identify patients who have a respectable tumour and can be cured by means of surgical intervention. Three-dimensional CT combined with CT angiography has the potential to provide all the critical information needed to characterise the lesion and plan the surgical procedure. Our 128-slice CT scanner provides pre-operative interactive display of a 3D model of the affected kidney and its vascular supply to the surgeons.
CT EVALUATION IN THORACIC OUTLET SYNDROME
Case: Right Subclavian Artery Occlusion
Courtesy: Dr. Nitin Pathak
Clinical Presentation:
Tingling and numbness in right upper limb. Mild discolouration of little finger.

Review of Literature
Subclavian angiography study is performed with the arm in overhead abduction.
Allows evaluation of the caliber and wall of subclavian artery, presence/absence of extrinsic compression, assessment of lesion extent and site, involvement of branch origin and evaluation of distal vessel flow
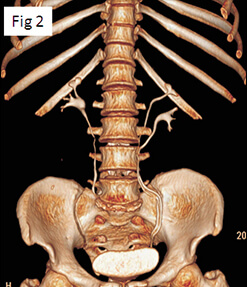
CONTRAST ENHANCED CT ANGIOGRAPHY OF THE ABDOMINAL AORTA AND LOWER LIMB ARTERIES
Case: Peripheral Arterial Disease
Courtesy: Dr. Rahul Patil

Clinical Presentation:
A 55 yr old patient with h/o peripheral arterial disease (PAD) and complaints of left lower limb claudication with ulcer.
Images and imaging findings:
Long segment intra-luminal filling defect, suggesting thrombotic occlusion of the left CIA and EIA, just distal to aortic bifurcation ( ).
• Distal-most EIA is reformed via multiple collaterals ( ). Arising from deep circumflex iliac, inferior epigastric-internal mammary pathway, superior rectal artery and lumbar arteries.
• Distal SFA and proximal and mid popliteal artery show long segment thrombotic occlusion, on the left side ( ). Distal left popliteal artery is reformed via collaterals ( ).
• Long segment thrombotic occlusion of right distal SFA ( ). Circumferential calcified plaque at SFA popliteal junction. Right popliteal artery reformed through collaterals ( ).
Review of Literature
Previously, DSA was the only established reliable imaging technique to quantify atherosclerotic disease load in patients with PAD. Advent of MDCTA now challenges this old gold standard, along with other non-invasive techniques such as magnetic resonance angiography (MRA).
Our 128-slice MDCT scanner offers better diagnostic interpretation and eloquent anatomical and pathological display of the entire arterial tree, non-invasively and at lowest radiation dose (iDose) optimizing maximum arterial enhancement, without venous contamination is a challenge in assessing distal run off of symptomatic limb
MULTISLICE CARDIAC CT IN CONGENITAL HEART DISEASES
Courtesy: Dr. Pankaj Sugaonkar
Cases: Anomalous Pulmonary Venous Return
Clinical Presentation
2D echo suggestive of pulmonary hypertension.




Case 1:
Cases: Tetrallogy of Fallot Pre and Postpperative Evaluation
Clinical Presentation
Cyanotic spells. 2D echo suggestive of right ventricular outflow tract obstruction, large VSD and overriding of the aorta.
Two post-operative cases showing RV-PA conduit and bilateral BT shunts are also documented.
Case: Congenital Aortic Abnormalities
Clinical Presentation
Differential pulse and blood pressure measurements.


REVIEW OF LITERATURE
CT angiography is important in the evaluation of pediatric congenital heart disease. It can be used for accurate depiction of complex cardiovascular anatomic features both before and after surgery.Evaluation of post treatment complications can also be performed.
CT facilitates assessment of extracardiac systemic and pulmonary arterial and venous structures.
Compared with the previous CT scan machines, 128 slice scanner yields images with better temporal and spatial resolution, greater anatomic coverage of the patient, more consistent enhancement with lesser volume of intravascular contrast material and high quality 2D reformation and 3-D reconstruction owing to acquisition of an isotropic data set. These are achieved with an additional advantage of reduced radiation dose to patient.
CT can be considered the first line imaging technique for evaluation of suspected vascular ring or sling, mapping of the aortopulmonary collateral arteries in patients with severe right ventricular outflow tract obstruction and evaluation of an anomalous pulmonary and systemic venous return.
CT CORONARY ANGIOGRAPHY
Case 1
Courtesy: Dr. Nitin Patki
Clinical Presentation:
Chest discomfort in a known hypertrophic cardiomyopathy patient.
To evaluate coronary tree.
CT coronary angiography was performed followed byDSA and stenting.
A subsequent one year follow up CT coronary angiography was performed.

CT CORONARY ANGIOGRAPHY
Case 2
Courtesy : Dr. M. S. Hiremath
Clinical Presentation:
Post CABG status.
Chest pain with positive stress test results.




Review of Literature
• Cardiac coronary angiography study allows ostium evaluation, presence/absence of vascular remodelling, percentage stenosis, characterisation of the plaque, evaluation of its extent and site, involvement of branch origin and evaluation of distal vessel. Limitations include very high calcium deposition within the vessel walls obscuring the lumen due to blooming artifacts.
• It has a negative predictive value in the range of 98% for ruling out significant instent restenosis.
• Assessment of bypass grafts and distal runoffs by invasive coronary angiography is cumbersome and often requires extra procedure time, contrast load, and radiation exposure. Cardiac CT provides 3D anatomy of grafts, is noninvasive and successfully visualises the grafts, anatomosis and distal ves