The Lockdown Edition Newsletter

Dr. Amit Zope
As all of you are aware, the last two months have been extremely unprecedented. Even
in the times of strict lockdown Star Imaging, continued its services by keeping two of our
centres operational 24 x 7.
From 1st May , all our centres are operational with due precautions for patients and doctors.
At present we are scheduling our appointments at timely interval to avoid crowding in waiting areas.
All doctors and staff are fully geared with protective measures and our COVID PROTOCOL is in place.
We are happy to present 5 cases with interesting findings that we have imaged during this lockdown period.
So please go ahead and read the LOCKDOWN TIMES.
Take care and stay safe.
Case 1
Clinical Summary
24 year old female presented with slowly progressive painless swelling in right cheek region.
Indolent symptoms since many years.
History of renal biopsy in childhood, likely for renal dysfuction.
Imaging Findings
- Large heterogeneously enhancing lesion overlying the right masseter muscle with extension into the buccal space. No infiltrative features or underlying bone involvement is noted.
-
Multiple intraparotid nodes are seen on the right side.
-
Soft tissue stranding of the overlying subcutaneous fat is notedwhich could be perilesional infammatory response.
-
Extensive bilateral multilevel cervical lymphadeno-pathy is noted.
-
Possibility of lymphogranulamatous disorder like Kimura's disease is likely.
USG Guided Biopsy
- Shows fibrous tissue with lymphoid follicular hyperplasia and reactive germinal centers. There is perivascular lymphocytic infiltrate with abundant eosinophils. Proliferation of blood vessels is noted.
-
No granuloma/ malignancy.
-
Right cheek biopsy - Lymphoid hyperplasia with eosinophilia, suggestive of Kimura disease.
Kimura disease
- Kimura disease (KD): Angiolymphoid proliferation with serum eosinophilia and elevated IgE
- Classic triad
- Subcutaneous and deep tissue masses of
head and neck
- Salivary gland masses: Parotid > submandibular
- Solid cervical lymphadenopathy
DD
- Nodal non-Hodgkin lymphoma
- Parotid mucoepidermoid carcinoma
- Nodal sarcoidosis
Key points and Treatment
- Unknown etiology; allergic and autoimmune theories favored and 50% have renal dysfunction
- Most common in young Asian male patients.
- Recommend renal function tests
Treatment
- Resection of mass lesion(s)
- Intralesional or oral steroids may temporize, though not cure
- Cyclosporine A reported to induce remission
- Consider radiotherapy for persistent/problematic lesions
- Observation alone if not symptomatic or disfiguring
Case 2
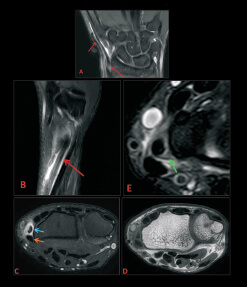
CECT abdomen and pelvis for suspected obstruction.
 Utility of the fat notch sign for adhesive bands as a cause of obstruction with risk of closed loop obstruction and strangulation
Utility of the fat notch sign for adhesive bands as a cause of obstruction with risk of closed loop obstruction and strangulation
FAT NOTCH SIGN - This sign reflects insinuation of mesenteric fat at an area of adhesions with focal caliber change. This has been described
in cases of small bowel obstruction related to adhesions and is a very specific fiinding of adhesive small bowel obstruction.

Case 2
61 year old male being evaluated for intestinal obstruction



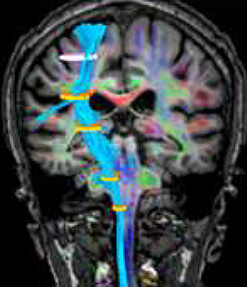
Case 3
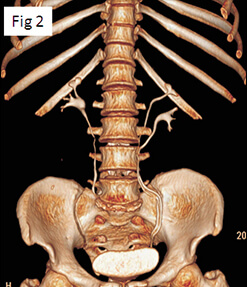
- Laparoscopic cervicopexy done
- Severe lower backache on left side.
- MRI to rule out sacral nerve injury.


Case 4
- 37 year young male
- Presented with shortness of breath.
- Was evaluated with 2D echo noncollapsible IVC. Large RA. Left pleural effusion and ascites.
- Cardiac CT and MR was performed for further evaluation.

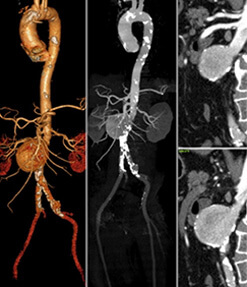
CONSTRICTIVE PERICARDITIS
- Cardiac CT has good spatial and temporal resolution, and multiplanar reconstruction abilities. It is the ideal technique for the evaluation of pericardial calcification and is very useful in preoperative planning.
- MRI is a valuable imaging tool--in both the morphologic and functional assessments for evaluation of small or loculated pericardial effusions, pericardial infiammation, and functional abnormalities caused by pericardial constriction.
- Pericardial thickening (> 4 mm) is an indicator of constriction in patients with the appropriate symptoms and signs of right heart failure. However, thickening does not always imply constriction.
- Long-standing constriction results in conical deformity of the ventricles. Other findings of constriction due to levated cardiac filling pressures are seen: biatrial enlargement; narrow atrioventricular groove; dilated SVC, IVC, and hepatic veins; pleural effusion; and ascites.
- Cardiac MRI evaluation allows distinguishing pericardial constriction from restrictive cardiomyopathy by demonstration of early diastolic septal flattening, feature specific for constriction.
- Constrictive pericarditis is treated with pericardectomy with complete regression of symptoms
Case 5
Case profile
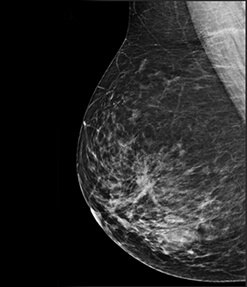
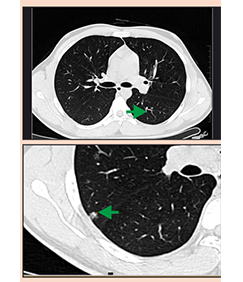
61 year old lady presented with dry cough for 1 year for which she was referred for HRCT thorax.

Further course
Incidentally noted was a left breast solid lesion which appeared to be irregular.
Mammography was advised which revealed a BIRADs V lesion in the left breast.
A core biopsy was performed.
Further preoperative work up revealed thickened endometrium with solid left adenexal region.
Patient was referred for MRI pelvis.


Final Diagnosis
- Infiltrating ductal carcinoma grade II breast (ER, PR Positive with equivocal HER2 status)
- High grade serous carcinoma FT - fallopian tube and ovary
- Benign endometrial polyp
Discussion
Patients with BRCA mutation have been found to have serous tubal intraepithelial carcinoma (STIC) in the fallopian tube and fimbria but not in the ovary and this is considered to be the precursor for high grade serous carcinomas (HGSCs). The proportion of HGSCs of ovarian and tubal origin is unknown because tumor growth in advanced stages of cancer obscures the primary site. In the present case; the lesion involving the fimbrial end of the fallopian tube and that of the left ovary can be visualized separately.